|
|
Sprengel's Deformity
Submitted by Samir Chedda, MD
General Considerations
- Most common congenital abnormality of the shoulder.
- Failure of normal descent of scapula from initial mid-cervical position to final thoracic position.
- Descent should occur between sixth and eight weeks gestation.
- Can occur unilateral or bilateral.
- If unilateral more common in left shoulder.
- Often occurs as part of Klippel-Feil Deformity (fusion of cervical vertebrae).
- Also can occur with absent or fused ribs, chest wall asymmetry, cervical ribs, and/or congenital scoliosis.
- 50% of cases have an omovertebral bone (bony or fibrous connection between scapula and the spinous process, lamina or transverse process of a vertebral body between C4 and C7)
Clinical Findings
- Presents with shoulder asymmetry and reduced abduction on physical exam
- Cavendish grading system:
- Grade 1: The deformity is very mild. The shoulders are almost level, and the deformity cannot be noticed with the clothes on.
- Grade 2: The deformity is mild. The shoulders are almost level, but the superomedial portion of the high scapula is visible as a lump.
- Grade 3: The deformity is moderate. It is visible, and the affected shoulder is elevated 2-5 cm higher than the opposite shoulder.
- Grade 4: The deformity is severe. The scapula is very high, with the superomedial angle at the occiput, with neck webbing.
Imaging Findings
- Conventional Radiographs
- Elevation of the affected scapula with the inferior angle rotated medially, pointing to the spine.
- CT (often with 3D reconstruction)
- Helpful for surgical planning, as can visualize more subtleties of bony margins
- Scapula is dysplastic, appearing smaller in the horizontal plane and larger in the vertical plane
- Inferior angle of scapula is rotated medially, causing glenoid to face inferiorly.
- Visualization of omovertebral connection if one is present.
Treatment
- Surgery indicated if severe cosmetic concerns or significant reduction in shoulder abduction in children less than age 6.
- Surgery relocates the scapula in the proper anatomical position and removes any omovertebral attachments
- Physical Therapy in less severe cases
Complications
- Untreated Sprengel's deformity can lead to shoulder muscle hypoplasia and atrophy, reduced shoulder function, and cosmetic disfigurement.
- Complications of surgery rarely include winging of scapula and brachial plexus injury
Prognosis


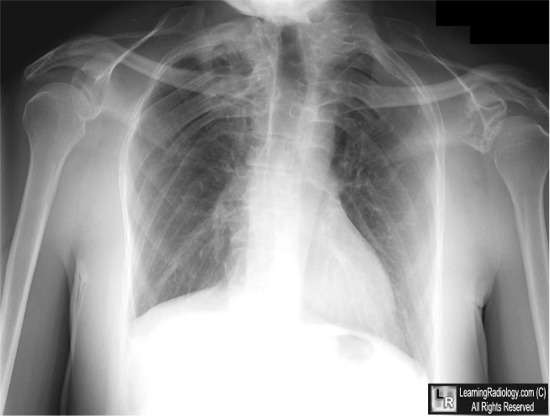
Sprengel's Deformity. Blue arrows point to elevation and medial angulation of both scapulae. There are
multiple rib anomalies (white arrows) including fused ribs. The red arrow points to the
medial orientation of the angle of the scapula.
For more information, click on the link if you see this icon 
For these same photos without the annotations, click here and here
Cavendish ME. Congenital elevation of the scapula. J Bone Joint Surg Br. Aug 1972;54(3):395-408.
Cho TJ, Choi IH, Chung CY, Hwang JK. The Sprengel deformity. Morphometric analysis using 3D-CT and its clinical relevance. J Bone Joint Surg Br. Jul 2000;82(5):711-8
Offiah, AC and Hall CM. Skeletal Radiology in Children: Non-traumatic and Non-malignant, Localized Disorders of the Skeleton. In Grainger and Allison's Diagnostic Radiology. 5th ed. Maryland Heights, MO: Churchill Livingstone; 2008: 1588.
Thaker MM, Feldman DS. Sprengel Deformity eMedicine
|
|
|

{kind=link}
{kind=link}